AVFCW – AVF Care Workshop
Maintaining Lifeline for the Lifetime
If you are reading this page, you are likely in one of these situations:
- You are a CKD patient preparing for dialysis and need a new AV fistula.
- You already have a fistula that has failed or never matured properly.
- Your dialysis unit has told you that your fistula flow is low and you may need angioplasty.
- Your fistula has suddenly stopped working.
- You have arm swelling, high pressures during dialysis, or repeated access problems.
At AVFCW, we focus exclusively on solving these problems — safely, systematically, and with long-term durability in mind.
For Patients Who Need a New AV Fistula
If you are approaching dialysis, creating the right fistula at the right time is critical. A properly planned AV fistula reduces infection risk, avoids catheter dependency, and improves long-term dialysis outcomes.
Before surgery, we evaluate:
- Your stage of kidney disease
- Vein and artery size (clinical and imaging assessment)
- Dominant arm and lifestyle factors
- Long-term dialysis planning
We create:
- Radiocephalic (wrist) AV fistula whenever possible
- Brachiocephalic AV fistula in the upper arm
- Brachiobasilic AV fistula with transposition when required
Most AV fistula surgeries are performed as daycare procedures. Patients typically go home the same day. The procedure is done under regional or local anesthesia in a controlled surgical setting.
After surgery, we follow a structured maturation protocol. A fistula is not declared successful just because it was created. It must mature properly, develop adequate flow, and be safe for dialysis cannulation.
We guide you through:
- When to start checking the thrill
- When dialysis can safely use the fistula
- Warning signs of delayed maturation
- When early intervention (angioplasty) may be required
Our goal is first-time success with long-term durability.

For Patients with a Failed or Non-Maturing Fistula
Many fistulas that “fail” are not truly failures — they are under-evaluated or untreated stenosis cases.
If your fistula:
- Never matured
- Has weak flow
- Cannot achieve adequate dialysis blood flow
- Has prolonged bleeding after dialysis
- Has frequent machine alarms
You likely have a narrowing (stenosis) that can often be treated.
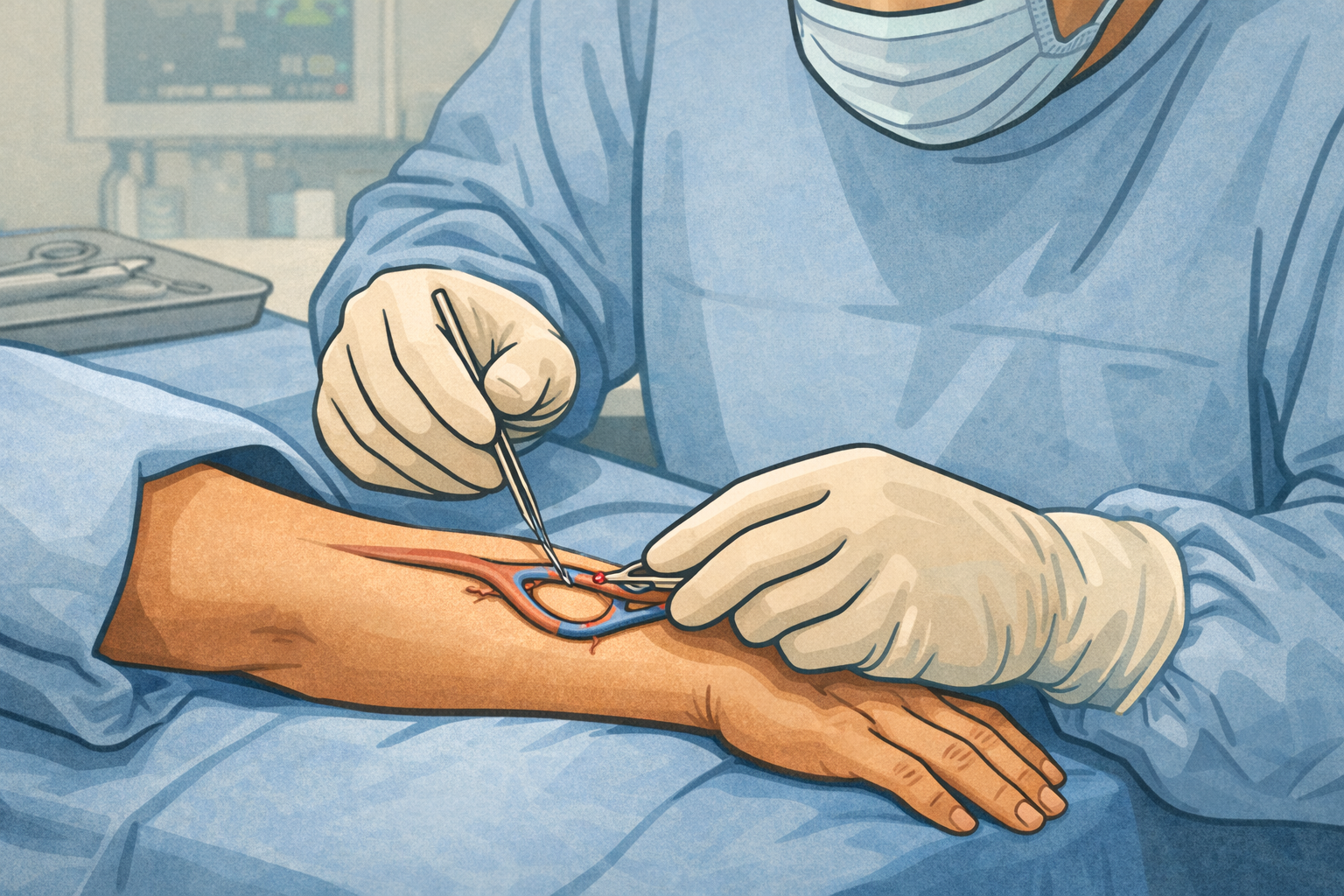
We perform:
- Detailed clinical assessment
- Targeted imaging when required
- Balloon angioplasty to open narrowed segments
- Surgical revision if anatomy demands it
Angioplasty is usually a minimally invasive, short-stay procedure, often completed the same day. Early treatment prevents thrombosis and preserves your access.
Timely intervention can convert a failing fistula into a durable one.
For Patients with a Failed or Non-Maturing Fistula
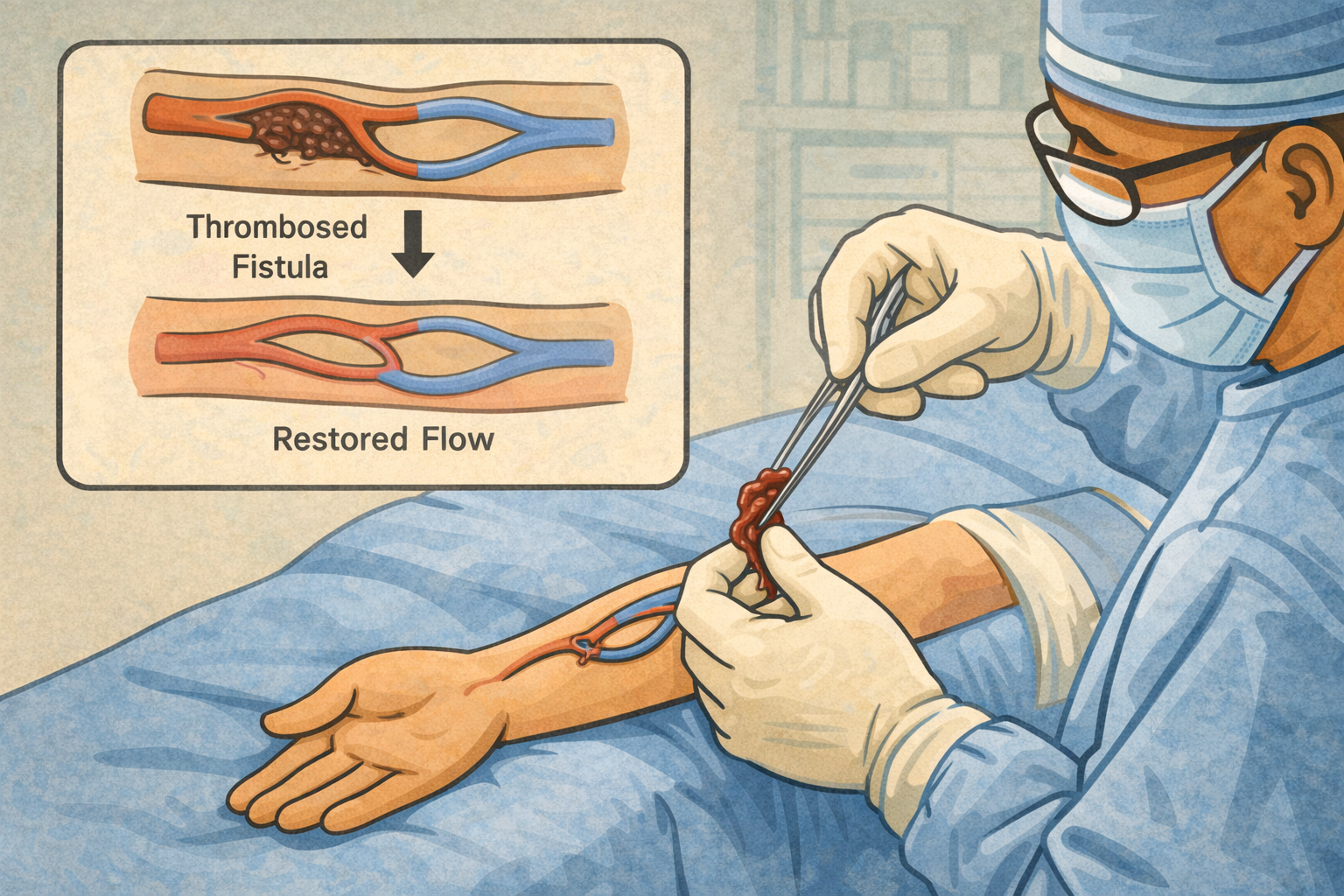
If you cannot feel the thrill and dialysis cannot use your access, this is urgent – but not always the end.
Many thrombosed AV fistulas can be salvaged if treated quickly.
We provide:
- Surgical thrombectomy
- Endovascular clot removal
- Identification and correction of the underlying stenosis
- Flow restoration strategies
The key principle: do not abandon the fistula without expert evaluation.
Emergency catheter insertion should not be the first option if salvage is possible.

For Patients with Recurrent Problems or Multiple Failures
Some patients have:
- Multiple previous fistula attempts
- Exhausted superficial veins
- Central venous stenosis
- Arm swelling with a functioning fistula
- Complex anatomy
These are not routine cases. They require specialized planning.
We perform:
- Complex redo fistula creation
- Basilic vein transposition
- Advanced flow correction procedures
- Central venous angioplasty
- Hybrid surgical–endovascular access reconstruction
- AV graft placement when native veins are unsuitable
Access planning in such cases is individualized and future-oriented.
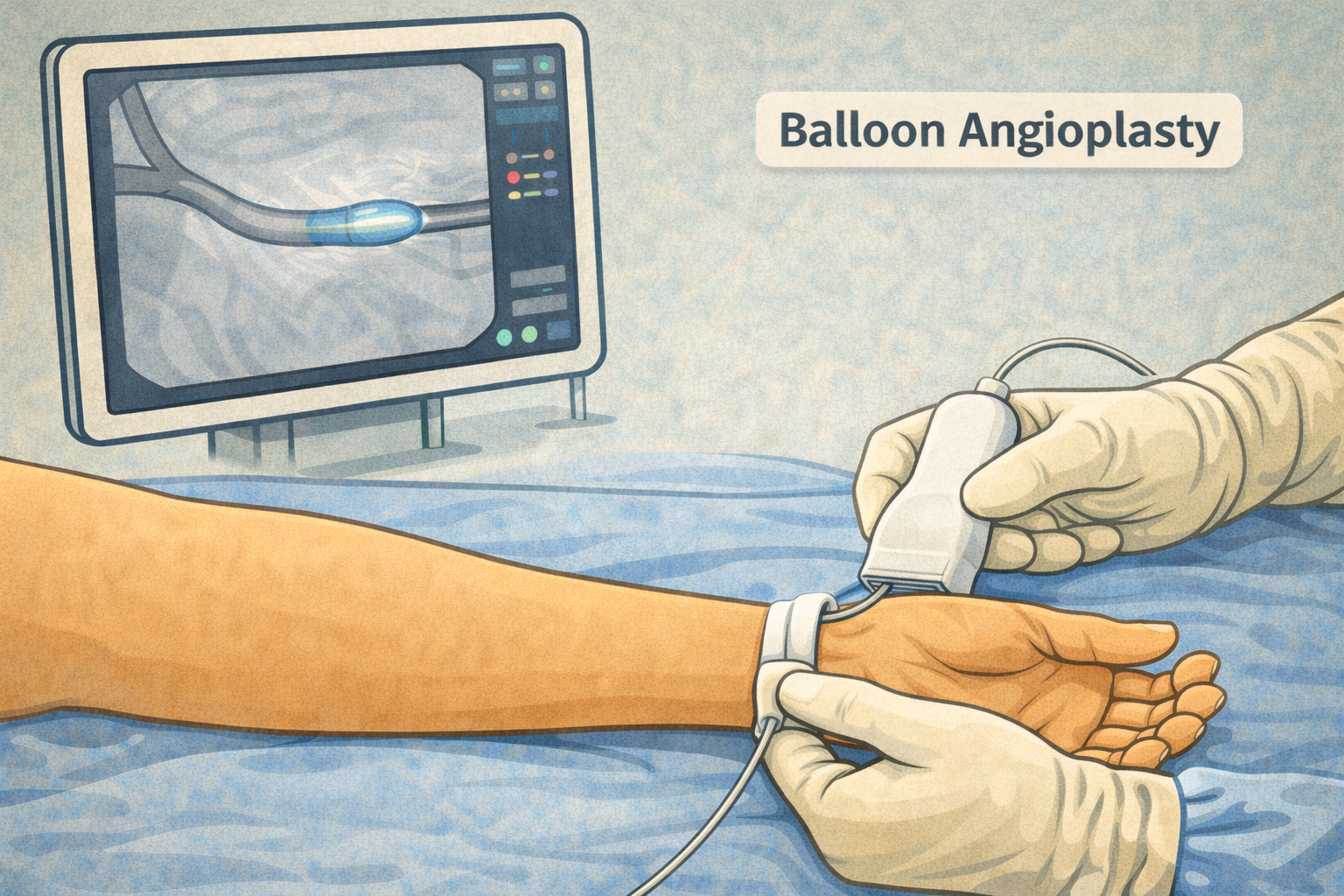
Angioplasty for AV Fistula Narrowing
If your nephrologist or dialysis unit has advised angioplasty, it usually means your fistula has a narrowing affecting flow.
Signs include:
- Rising venous pressures
- Reduced dialysis adequacy
- Prolonged bleeding
- Weak thrill
- High-pitched bruit
We perform AV fistula angioplasty to restore flow and prevent clotting. In selected cases, advanced balloon technologies may be used depending on lesion characteristics.
Angioplasty is not a failure — it is part of long-term fistula maintenance.
Early angioplasty prevents emergency thrombosis.
What Makes Our Approach Different
At AVFCW, surgery is only the beginning.
We emphasize:
- Structured maturation monitoring
- Patient training in self-AV fistula examination
- Stethoscope-based monitoring techniques
- Early detection of acoustic changes
- Pre-emptive angioplasty rather than emergency salvage
- Long-term follow-up continuity
Many of our patients have functioning AV fistulas for 10–15 years with proper surveillance and timely intervention.
Our Commitment
Whether you need your first fistula, a salvage procedure, or long-term surveillance support, our mission remains the same:
Maintaining Lifeline for the Lifetime
If you would like next, I can:
- Create a patient decision-tree section (“Which category do you fall into?”)
- Add a short FAQ below this services page
- Or convert this into separate SEO landing pages for “AV Fistula Surgery”, “AV Fistula Angioplasty”, and “Failed AV Fistula Treatment.”

AVF Care Workshop – On Demand
We also conduct AV Fistula Care Workshops for dialysis centers, nephrology units, patient groups, and healthcare institutions.
These workshops cover:
- Understanding AV fistula types
- Cannulation safety
- Recognizing early signs of failure
- Self-AV fistula examination using stethoscope
- Preventing thrombosis
- When to seek intervention
Workshops are conducted on a request-based model and can be customized for patients, caregivers, nurses, or doctors.
If you would like to organize an AVF Care Workshop in your center or community, connect with us to know more.

