EDUCATION CORNER
Haemodialysis depends on safe and reliable vascular access. Your AV fistula or dialysis catheter is not just a medical device — it is your lifeline. Understanding how it works, how to protect it, and when to seek help can prevent serious complications and extend its lifespan.
1. What Is AV Access and Why Is It Your Dialysis Lifeline?
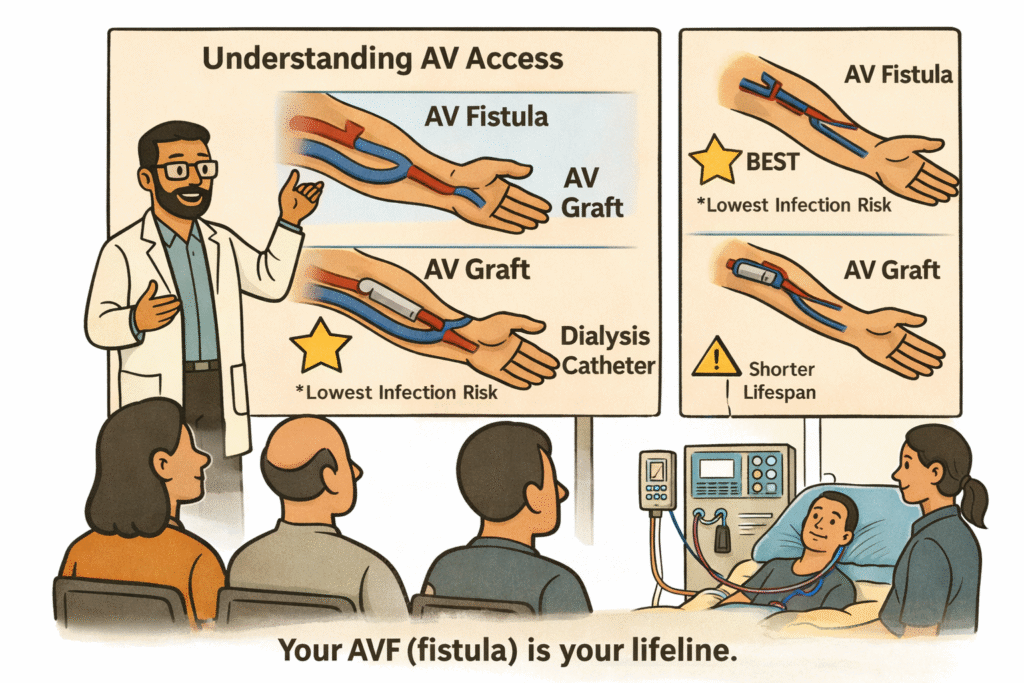
AV access is the pathway through which blood is removed, purified, and returned during haemodialysis. There are three main types of dialysis access:
- AV fistula — the safest and most durable option.
- AV graft — a synthetic connection between an artery and a vein.
- Dialysis catheters (temporary line or Permacath) — usually used as a bridge.
An AV fistula, when properly created, matured, and supervised, offers the lowest infection rate, the best dialysis efficiency, and the longest survival. Whenever possible, a fistula-first approach provides the safest long-term strategy.
2. Permacath for Dialysis: How Long Can You Use It Safely?
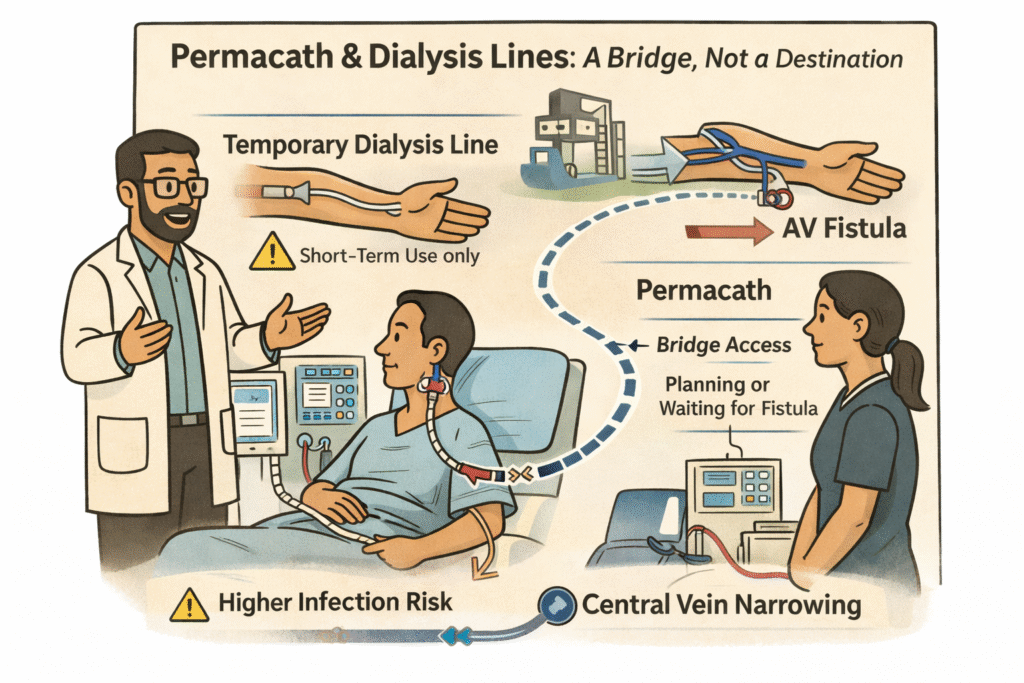
When dialysis must begin urgently and a fistula is not yet available, a catheter is inserted into a large vein.
A temporary dialysis line is used in emergency situations and carries a higher infection risk.
A Permacath is a tunnelled dialysis catheter placed under the skin and into a central vein, usually in the neck. It is more stable than a temporary line but still carries risks of infection, clotting, and central vein narrowing.
A Permacath is best understood as a strategic bridge. It allows safe dialysis while a fistula is being planned or matured. In complex cases, it may also provide time to improve nutrition, treat infection, optimise heart function, and stabilise overall health before attempting another access surgery.
If you develop fever, chills, redness at the exit site, or poor dialysis flow while using a Permacath, seek urgent medical review. Catheter blockage may require clot-dissolving medication or catheter exchange. Infection may require antibiotics and, in some cases, catheter removal.
Long-term catheter dependence increases the risk of complications. Timely fistula planning therefore remains essential.
3. How Is an AV Fistula Created, and What Does Maturation Mean?
An AV fistula is created by surgically connecting an artery to a vein. The increased blood flow causes the vein to enlarge and strengthen over time. This preparation phase is called maturation and usually takes 4 to 8 weeks.
A mature fistula should have a strong, continuous vibration (called a thrill), good blood flow, and adequate size. Importantly, it should also lie close enough to the skin surface to allow safe needle insertion — ideally within about 4 to 6 millimetres of the skin.
Helping your fistula mature: Your doctor may recommend gentle hand-grip exercises (such as squeezing a soft ball for 10–15 minutes, three to four times a day) to encourage vein enlargement. Always follow your surgeon’s specific instructions regarding when to start and how often to exercise.
What If Your Fistula Is “Deep”?
Sometimes patients are told their fistula is “deep.” This may happen if the vein lies beneath thicker fatty tissue, if it has not enlarged adequately, or if the arm is swollen. A healthy but deep fistula can often be corrected with a minor procedure called superficialisation or transposition, which brings the vein closer to the surface. If the vein is small, balloon-assisted maturation (angioplasty) may help it enlarge. In cases where arm swelling is caused by central vein stenosis, treating the narrowing may improve the situation.
A proper evaluation by a vascular access specialist determines the safest correction strategy.
4. What If My AV Fistula Has Not Matured on Time?
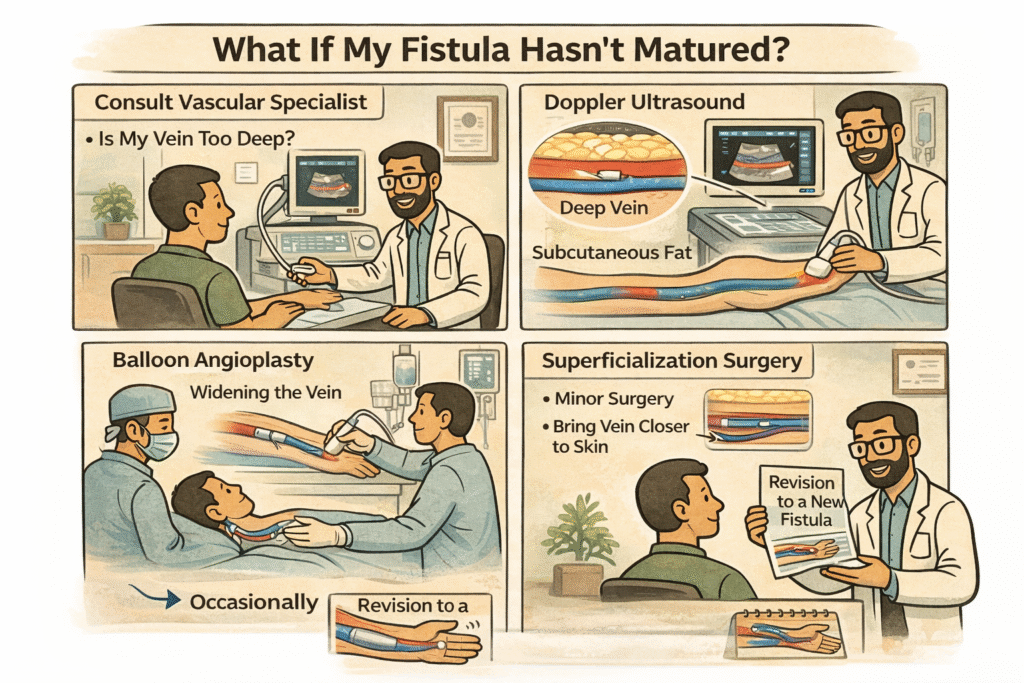
A fistula that appears slow to mature does not necessarily indicate failure. Ultrasound evaluation may reveal narrowing near the surgical connection. Balloon angioplasty can improve blood flow and promote maturation. Occasionally, minor surgical correction is required. In rare cases, a new fistula may need to be created at a different site.
Early detection and timely intervention significantly improve success rates. If your fistula has not matured within the expected timeframe, speak with your vascular access team rather than assuming it has failed.
5. Starting Dialysis from a Fistula: What to Expect During Your First Sessions
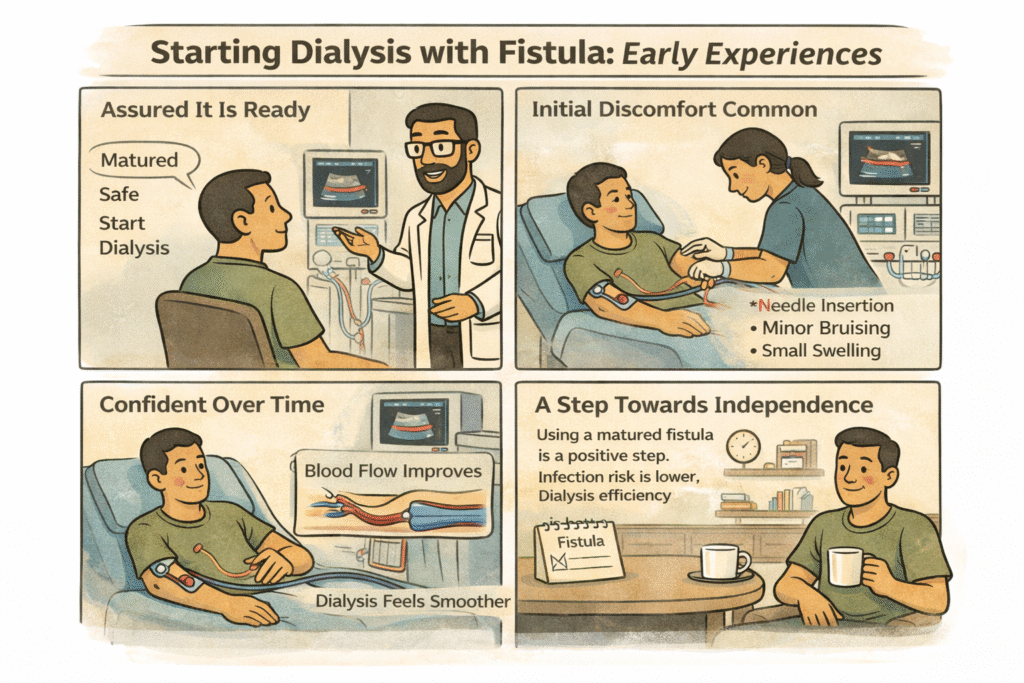
Dialysis should begin only when your doctor confirms that the fistula is ready. Starting too early can damage the vein and compromise long-term function.
During the first few sessions, mild discomfort, slight bruising, or minor swelling may occur. This usually settles as the vein adapts to repeated use. Compared to catheter-based dialysis, fistula-based dialysis offers better blood flow, fewer infections, and improved long-term safety.
Needle technique matters: Your dialysis team should use the rope-ladder technique (rotating needle sites along the length of the fistula) or, where appropriate, the buttonhole technique (using the same site with blunt needles). Consistent, careful cannulation protects your fistula from unnecessary damage.
6. Why Is My Fistula Arm Swollen After Dialysis? Causes and When to Worry
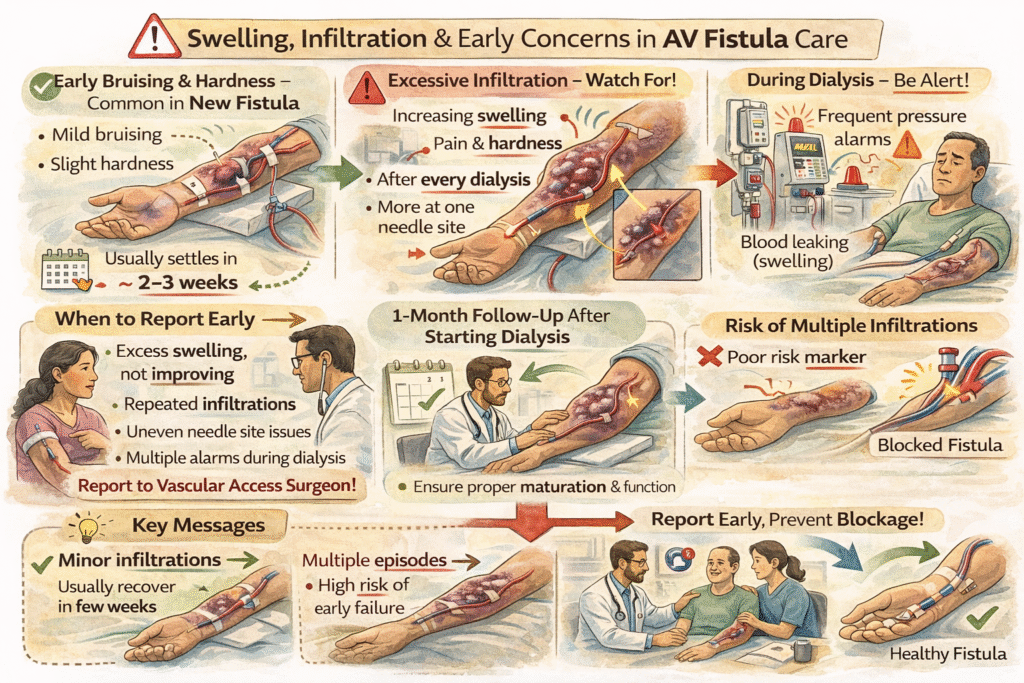
If swelling or bruising develops around a needle site after dialysis, it may be caused by infiltration — a situation where blood leaks into the surrounding tissue. Inform the dialysis team immediately. The area may need to rest before it can be reused.
However, swelling of the entire arm — particularly if one arm appears noticeably larger than the other — should not be ignored. This may indicate central vein narrowing (stenosis) and requires specialist evaluation.
Persistent pain, repeated difficulty with needle insertion, or progressively increasing swelling all warrant medical review.
7. Why Do AV Fistulas Stop Working? Warning Signs You Should Watch For
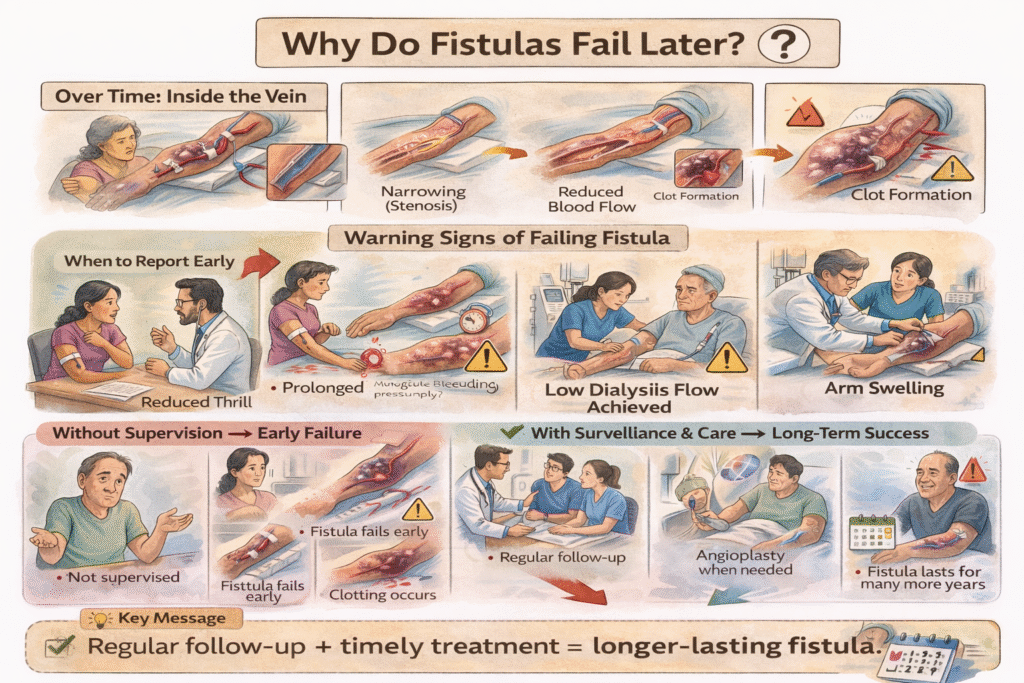
Over time, fistulas may develop narrowing (stenosis) within the vein. If left untreated, this reduces blood flow and can eventually lead to clotting — which may cause permanent fistula loss.
Warning signs that your fistula may be developing a problem include:
- Reduced or absent thrill (the vibration you normally feel)
- Prolonged bleeding after dialysis needles are removed
- Difficulty achieving adequate blood flow during dialysis
- New or worsening arm swelling
Most fistulas fail prematurely when they are not monitored regularly. With structured clinical surveillance — such as periodic ultrasound assessments every 3 to 6 months — and timely angioplasty when needed, the same fistula can function for many years longer than one that is neglected.
8. AV Fistula Lifespan: How Many Years Can It Last?
It is difficult to predict exact fistula longevity at the time of surgery. Lifespan depends on vein quality, maturation success, blood pressure stability, dialysis technique, and the consistency of follow-up surveillance.
A well-matured and regularly supervised fistula often lasts 3 to 5 years or longer. Some fistulas function well for a decade or more under expert care. Without regular monitoring, even a good fistula may fail prematurely due to undetected narrowing or other correctable problems.
The single most important factor in extending fistula life is consistent, structured surveillance by your vascular access team.
9. Swollen or Bulging Fistula: Understanding Aneurysms and the Pinch Sign
Over time, some fistulas become enlarged and may appear swollen or bulging. This is called aneurysmal change. Most enlarged fistulas are not immediately dangerous — many look cosmetically prominent but continue to function safely for years.
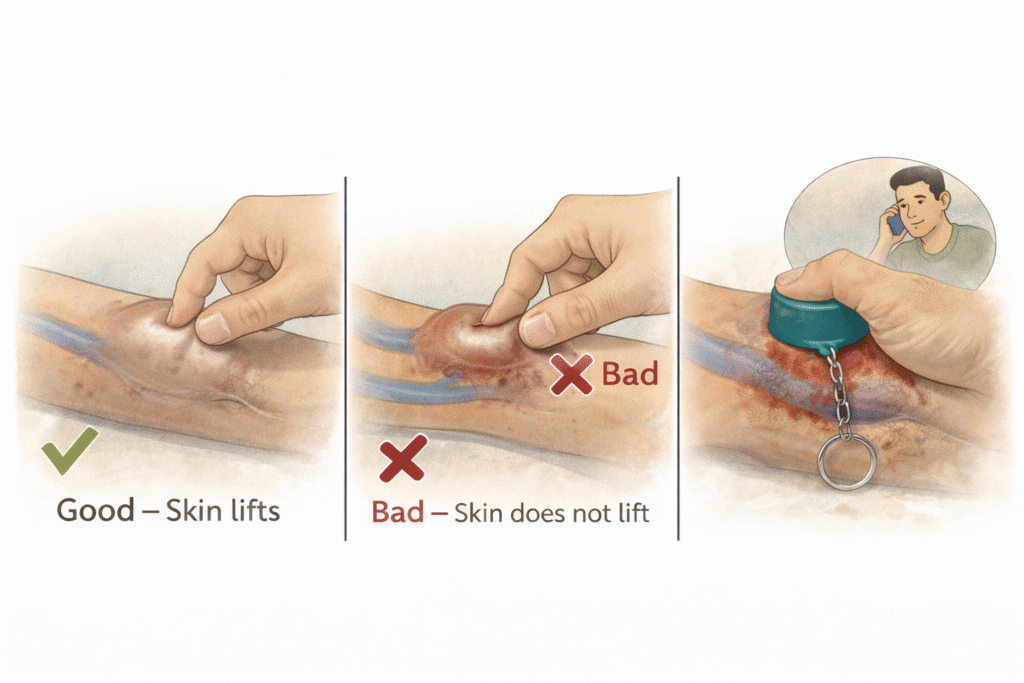
Certain features, however, make a swollen fistula high-risk. If the swelling is associated with very high blood flow, shiny or thin skin, ulceration, or areas where the skin cannot be gently pinched, the situation becomes concerning.
The pinch sign is an important self-check. If you cannot gently pinch and lift the skin over a swollen segment of your fistula, it suggests the skin has become dangerously thin. Such areas should never be punctured for dialysis.
Scab formation over a fistula is particularly dangerous. A thick, dark scab over a bulging area may conceal a weakened skin surface. If such a scab accidentally opens, it can cause sudden, heavy bleeding because the fistula carries high-pressure blood. These areas require urgent medical evaluation.
.
10. Fistula Bleeding Emergency: What to Do Immediately
Severe bleeding from a fistula is rare but can be life-threatening if not managed promptly.
If bleeding occurs, follow these steps:
- Apply firm, direct pressure immediately over the bleeding point.
- Use a clean cloth or gauze pad.
- Maintain steady, continuous pressure without releasing.
- Call for emergency medical help while maintaining pressure.
In an emergency situation, even a clean bottle cap wrapped in cloth can be used to apply focused pressure over the bleeding point until medical help arrives. This concentrated pressure can temporarily control bleeding more effectively than a flat hand.
Commercially available fistula safety caps are designed for similar emergency compression. Patients and families should be educated about emergency bleeding control, especially if aneurysmal changes or thin skin are present.
Any episode of spontaneous or unexpected bleeding from a fistula requires urgent vascular evaluation.
11. AV Fistula Failed Multiple Times? Understanding Complex Access Options
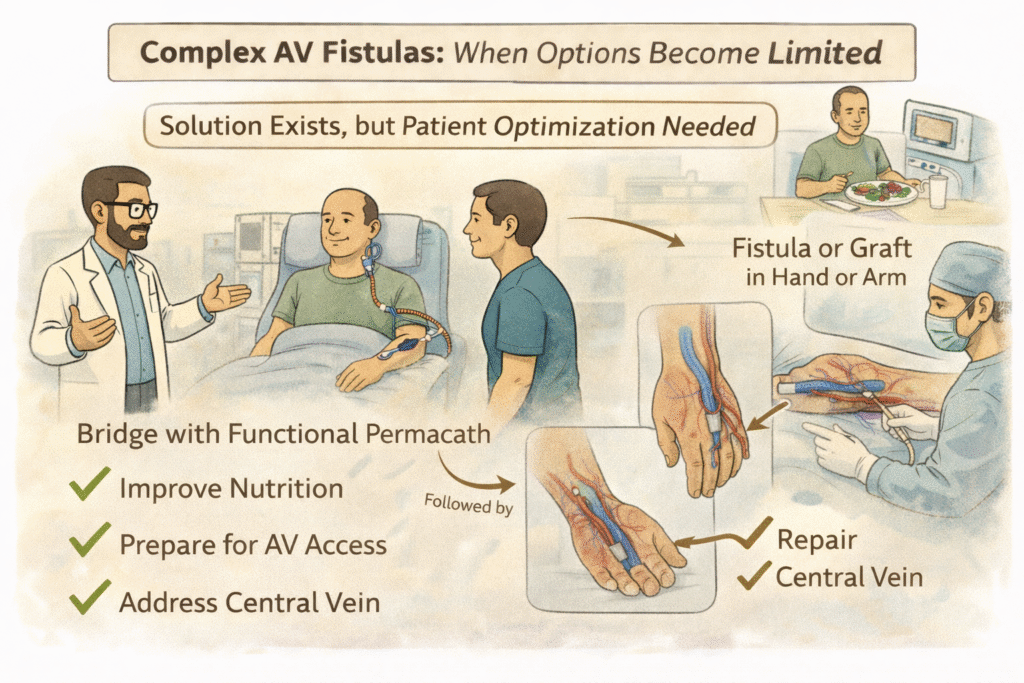
A complex AV fistula situation arises when patients have experienced multiple failed accesses, blocked central veins, thrombosed veins, or limited remaining sites for access creation.
In such cases, careful reassessment is crucial. Sometimes the safest approach is not to immediately attempt another surgery. Instead, maintaining a well-functioning Permacath for a few months while optimising nutrition, correcting anaemia, improving cardiac function, and stabilising overall health may significantly improve the chances of future surgical success.
Access surgery is not solely about surgical skill — it is equally about what the body can physiologically support. After thorough medical optimisation and proper vascular imaging, many patients who were previously considered to have “no options” may again become candidates for advanced fistula creation.
Complex access requires strategic planning, patience, and individualised decision-making between you and your vascular access team.
.
12. How to Examine Your AV Fistula: A Daily Self-Check Guide
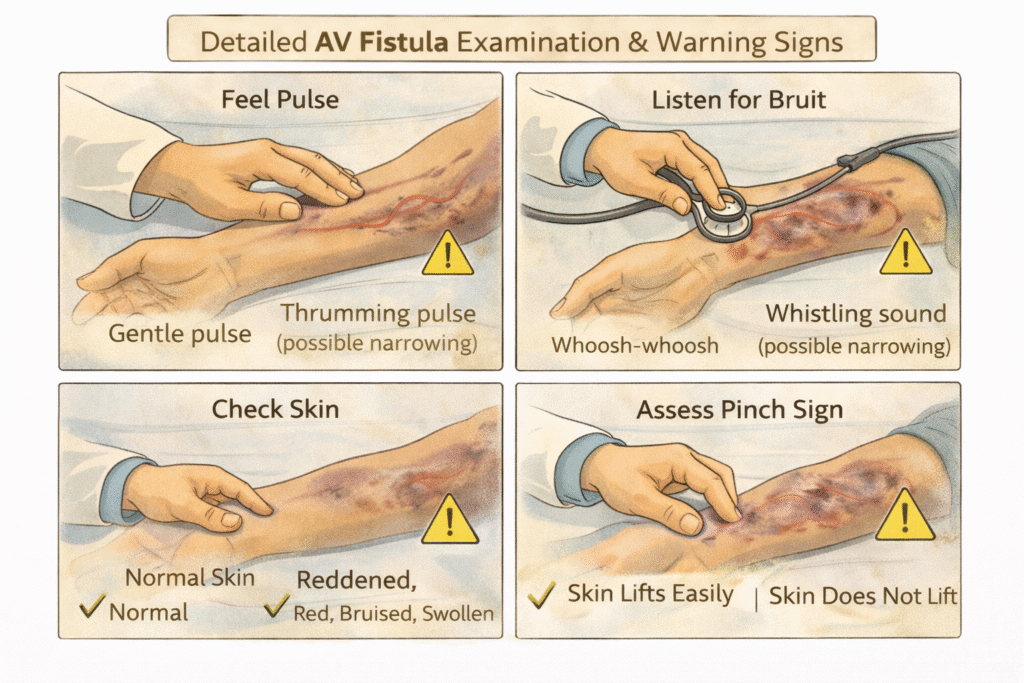
Your fistula should always have a continuous vibration (thrill) when touched gently. A sudden loss of this thrill is an emergency — contact your medical team immediately.
Consolidated Warning Signs — When to Seek Urgent Medical Attention:
- Sudden loss of thrill or pulse in the fistula
- Prolonged bleeding after dialysis (more than 20–30 minutes)
- Redness, warmth, or pus around needle sites or along the fistula
- Severe or worsening pain in the fistula arm
- Hard, firm areas or lumps along the vein
- Persistent or non-healing scabs over the fistula
- Swelling of the entire arm (especially if one arm is noticeably larger)
- Cold fingers, numbness, or tingling in the fistula hand
- Shiny, thinning skin over swollen or bulging segments
- Any spontaneous bleeding from the fistula
Early reporting allows timely intervention and often prevents permanent access loss. Make it a habit to check your fistula at least once every day.
13. Basilic Vein Transposition (BVT): A Powerful Native Vein Option When Standard Fistulas Are Not Possible
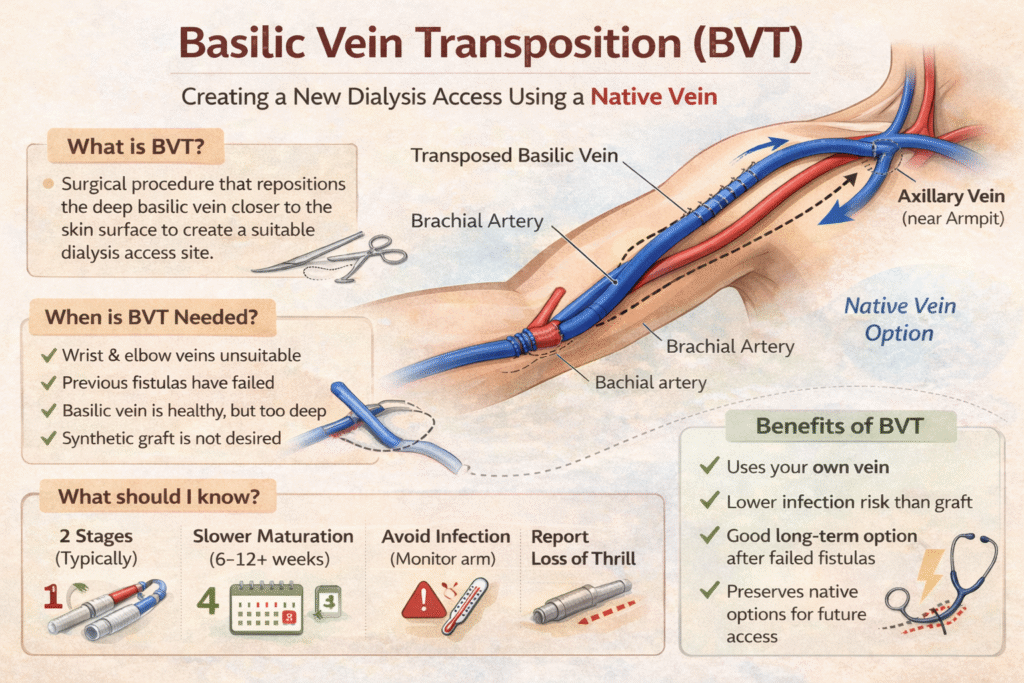
Many patients are told that their wrist or elbow veins are not suitable for creating a standard AV fistula. This does not automatically mean that a synthetic graft is the only remaining option. In many cases, another natural vein called the basilic vein can be used to create a durable, long-term fistula.
The basilic vein runs along the inner side of the upper arm. Unlike the cephalic vein (used in radiocephalic or brachiocephalic fistulas), the basilic vein lies deeper under the muscle and cannot be used for direct needle puncture in its natural position. It is, however, often healthy and of good calibre.
Basilic Vein Transposition (BVT) is a surgical technique in which this deep vein is connected to the artery and then repositioned closer to the skin surface so that it can be safely accessed for dialysis.
When Is Basilic Vein Transposition Recommended?
BVT is typically considered when:
- Both wrist (radiocephalic) and elbow (brachiocephalic) fistulas are not possible
- The cephalic vein is too small or has already thrombosed
- Previous fistulas have failed
- A durable native vein option is preferred over a synthetic graft
Many patients who are told they “have no vein options” may still be candidates for a well-planned BVT after proper ultrasound mapping of the arm veins.
How Is BVT Performed?
BVT can be performed in one or two stages, depending on the vein size and the patient’s overall condition.
Stage 1: In the first stage, the basilic vein is connected to the brachial artery. The vein is left in its deeper position to allow it to arterialise and enlarge over several weeks.
Stage 2: After the vein has matured and strengthened, a second surgery is performed. The matured basilic vein is carefully mobilised and brought closer to the skin surface, allowing safe needle insertion for dialysis.
In selected patients with suitably large veins, a single-stage BVT may be possible. However, a two-stage approach often improves maturation rates and long-term durability.
What Are the Advantages of BVT?
- Uses your own vein — no synthetic material is required
- Lower infection risk compared to a synthetic graft
- Better long-term survival than many graft options
- A strong option for patients with failed wrist or elbow fistulas
What Should Patients Know About Recovery?
Because BVT involves more extensive surgical dissection than a simple wrist fistula, swelling may be slightly greater in the early postoperative period. Once the fistula has matured, however, it often functions very well.
Follow-up is essential to monitor maturation and confirm that the vein has become suitable for dialysis. BVT is an important part of advanced access planning and often allows patients to avoid moving prematurely to a synthetic graft.
14. AV Graft for Dialysis: What to Know If Your Doctor Recommends a Graft
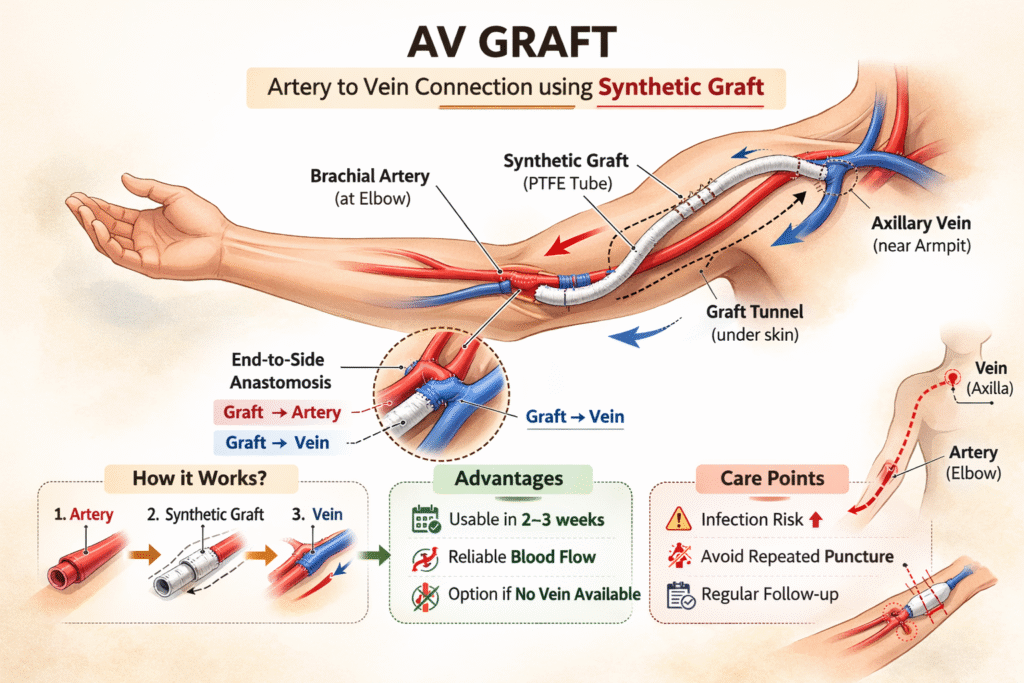
An AV graft is a dialysis access created using a soft synthetic tube placed under the skin to connect an artery to a vein. Unlike a fistula, which uses your own vein, a graft uses artificial material to provide a pathway for blood flow. This procedure can be performed in the forearm, the upper arm, or other sites; however, a connection between the artery at the elbow and the vein in the axilla (armpit area) is the most common configuration.
When Are AV Grafts Recommended?
- Natural veins are too small or damaged for a fistula
- Previous fistulas (including BVT) have failed
- The basilic vein is unsuitable
- Rapid dialysis access is needed
- Central vein anatomy limits native access options
Being advised to have a graft does not mean that previous treatment has failed. It means that, based on your current vascular condition, a graft may provide the safest and most practical dialysis access.
How Does an AV Graft Work?
The synthetic tube carries arterial blood into the vein. During dialysis, needles are inserted directly into the graft material. Grafts can typically be used earlier than fistulas (often within 2 to 3 weeks after surgery), feel firmer than natural veins, and provide reliable blood flow.
What Are the Risks of AV Grafts?
Because grafts are made of synthetic material, they carry a slightly higher infection risk than fistulas, are more prone to clotting, and may require more frequent maintenance procedures such as angioplasty. With structured surveillance and timely intervention, however, grafts can function well for years.
How Is Graft Cannulation Different from Fistula Cannulation?
A graft does not stretch like a natural vein. It feels firm and uniform to the touch. Repeated puncture at the same site can weaken it, so rotation of needle sites using the rope-ladder technique is extremely important. The buttonhole technique is generally not used with grafts.
What Should You Monitor in a Graft?
Report any of the following promptly: redness or warmth around the graft, fever, swelling around needle sites, sudden loss of thrill, prolonged bleeding, or unusual pain or firmness. Early detection of problems significantly improves graft longevity.
How Long Does a Graft Last?
Graft lifespan varies depending on patient health, blood pressure stability, cannulation technique, and the regularity of follow-up. Grafts typically require more maintenance than fistulas, but with proper supervision, they can provide reliable dialysis access for an extended period.
Important: Whenever possible, native vein fistulas (including BVT) are the preferred option. However, AV grafts are valuable and appropriate alternatives when natural veins are not suitable.
The key is not which type of access you have — the key is how well it is supervised, protected, and maintained.
15. Living with Dialysis: Protecting Your Lifeline and Your Mental Well-Being
Never allow blood pressure measurement, injections, or blood draws from your fistula arm. Avoid tight clothing, heavy lifting, and direct trauma to the access site. Early access planning during the course of chronic kidney disease significantly reduces the need for emergency catheter placement.
Dialysis also affects emotional health. Anxiety about fistula failure, repeated procedures, and visible physical changes can cause stress, frustration, or depression. Education, structured follow-up programmes, family support, and open communication with your healthcare team all contribute to long-term confidence and resilience.
A supervised fistula lasts longer.
An informed patient protects their access better.
And a protected access protects life.
Frequently Asked Questions About AV Fistula and Dialysis Access
How do I know if my AV fistula is working properly?
Place your fingers gently over the fistula. You should feel a continuous vibration (thrill) and hear a soft buzzing sound. If this vibration suddenly disappears or changes, contact your medical team immediately.
Can I exercise with an AV fistula?
Light exercise is generally safe and beneficial. Gentle hand-grip exercises can help your fistula mature. Avoid heavy lifting, contact sports, or any activity that puts direct pressure on the fistula arm. Always consult your doctor about specific activities.
How often should my fistula be checked by a doctor?
Routine surveillance — typically an ultrasound assessment every 3 to 6 months — is recommended. Your vascular access team may adjust this schedule based on your individual situation.
What should I do if my fistula stops buzzing?
A sudden loss of thrill (buzzing sensation) may indicate clotting. This is an emergency. Contact your vascular access team or visit your nearest emergency department immediately. Early intervention can sometimes save the fistula.
Is a Permacath permanent?
Despite its name, a Permacath is not intended for permanent use. It is a tunnelled catheter designed as a temporary bridge while a fistula is being planned, created, or matured. Long-term catheter use increases the risk of infection and central vein damage.
Why was I told I need a graft instead of a fistula?
A graft is recommended when your natural veins are not suitable for fistula creation. This may be due to small vein size, previous failed fistulas, or vein damage. A graft is a safe and effective alternative that allows reliable dialysis access.

